Overview of Labor
What is labor?
Labor is a series of continuous, progressive contractions of the uterus which help the cervix to open (dilate) and to thin (efface), allowing the fetus to move through the birth canal. Labor usually starts two weeks before or after the estimated date of delivery. However, no one knows exactly what triggers the onset of labor.
What are the signs of labor?
Signs of labor vary from woman to woman, as each woman experiences labor differently. Some common signs of labor may include:
Bloody show
A small amount of mucus, slightly mixed with blood, may be expelled from the vagina indicating a woman is beginning labor.Contractions
Contractions (uterine muscle spasms) occurring at intervals of less than ten minutes are usually an indication that labor has begun; contractions may become more frequent and severe as labor progresses.Rupture of amniotic sac (bag of waters)
Labor sometimes begins with amniotic fluid gushing or leaking from the vagina. Women who experience a rupture of the amniotic sac should contact their doctor or midwife immediately. The majority of women with ruptured membranes go into labor within 24 hours. If labor still has not begun after 24 hours, a woman may be hospitalized for labor to be induced. This step is often taken to prevent infections and delivery complications.
If a woman feels unsure if labor is beginning, she should always call her doctor or midwife.
What are the different stages of labor?
Each labor is different. However, labor typically is divided into three stages:
First Stage |
The first phase of the first stage of labor is called the latent phase, when contractions are becoming more frequent (usually 5 to 20 minutes apart) and somewhat stronger. However, discomfort is minimal. The cervix dilates (opens approximately three or four centimeters) and effaces (thins out). Some women may not recognize that they are in labor if their contractions are mild and irregular. The latent phase is usually the longest and least intense phase of labor. The mother-to-be is usually admitted to the hospital during this phase. Pelvic exams are performed to determine the dilation of the cervix. The second phase of the first stage (active phase) is signaled by the dilation of the cervix from 4 to 7 centimeters. Contractions become longer, more severe, and more frequent (usually 3 to 4 minutes apart). The third phase is called transition and is the last phase. During transition, the cervix dilates from 8 to 10 centimeters. Contractions are usually very strong, lasting 60 to 90 seconds and occurring every few minutes. Most women feel the urge to push during this phase. In most cases, the active and transition phases are shorter than the latent phase. |
|---|---|
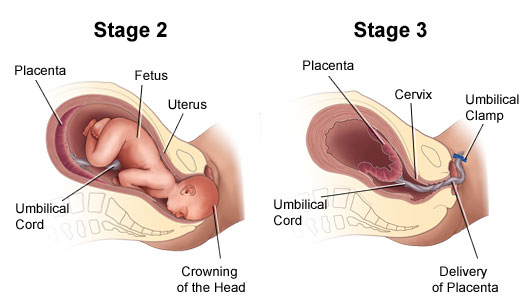
Second Stage |
The second stage of labor begins when the cervix is completely opened and ends with the delivery of the baby. The second stage is often referred to as the "pushing" stage. During the second stage, the woman becomes actively involved by pushing the baby through the birth canal to the outside world. When the baby's head is visible at the opening of the vagina, it is called "crowning." The second stage is shorter than the first stage, and may take between 30 minutes to two hours for a woman's first pregnancy. |
Third Stage |
After the baby is delivered, the new mother enters the third and final stage of labor--delivery of the placenta (the organ that has nourished the baby inside of the uterus). This stage usually lasts just a few minutes and involves the passage of the placenta out of the uterus and through the vagina. |
Each labor experience is different and the amount of time in each stage will vary. However, labor in a first pregnancy usually lasts about 12 to 14 hours. Labor is generally shorter for subsequent pregnancies.
Induction of labor
In some cases, labor has to be "induced," which is a process of stimulating labor to begin. The reasons for induction vary. Labor induction is not done before 39 weeks of pregnancy unless there is a problem. Some common reasons for induction include the following:
The mother and/or fetus are at risk
The pregnancy has continued too far past the due date
The mother has preeclampsia, eclampsia, or chronic hypertension
Diagnosis of poor growth of the fetus
Some common techniques of induction include the following:
Inserting vaginal suppositories that contain prostaglandin hormone to stimulate contractions.
Administering an intravenous infusion of oxytocin (a hormone produced by the pituitary gland that stimulates contractions) or similar drug.
Rupturing (artificially) the amniotic sac (bag of waters).
Care at the hospital during labor
When a woman arrives at the hospital in labor, the nursing staff may perform a physical examination of the abdomen to determine the size and position of the fetus, and an examination of the cervix. In addition, the nursing staff may check the following:
Blood pressure
Weight
Temperature
Frequency and intensity of contractions
Fetal heart rate
Urine and blood samples
Intravenous fluids are sometimes given during labor. The intravenous line, a thin plastic tube inserted into a vein (usually in the patient's forearm), can also be used to administer medications. Intravenous fluids are usually given once active labor has begun, and are also needed when a woman has epidural anesthesia.
The fetus, too, is carefully monitored during labor. A monitor placed over the mother's abdomen will keep track of the fetal heart rate.
What are pain management options during labor?
A woman has many options for managing the discomforts that occur during labor and the birth of her baby. Generally, mothers and their doctors or midwives want to use the safest and most effective method of pain relief for both mother and baby. The choice will be determined by:
Patient and family preference
The health of the patient
The health of fetus
The doctor's recommendation
There are three main types of pain management for labor and birth:
Nonmedicated measures--provide comfort and relieve stress, sometimes called natural childbirth. Many women learn special techniques to help them feel more comfortable and in control during labor and birth. Some of these techniques include:
Relaxation--techniques such as progressive relaxation, in which various muscle groups are relaxed in series, can help a woman detect tension and be better able to release that tension
Touch--this may include massage or light stroking to relieve tension. A jetted bath or a shower during labor may also be effective ways to relieve pain or tension. Ask your doctor before taking a tub bath in labor.
Heat or cold therapy--used to help relax tensed or painful areas, such as a warmed towel or a cold pack
Imagery--technique of using the mind to form mental pictures that help create relaxed feelings
Meditation or focused thinking--focusing on an object or task, such as breathing helps direct the mind away from the discomforts
Breathing-techniques using different patterns and types of breathing to help direct the mind away from the discomforts
Positioning and movement--many women find changing positions and moving around during labor helps relieve discomfort and may even speed labor along. Rocking in a rocking chair, sitting in the "Tailor sit" position, sitting on a special "birthing ball," walking, and swaying may be helpful. Your labor nurse or doctor can help you find comfortable positions that are also safe for you and your baby.
Analgesics--medications to relieve pain such as meperidine. The smallest dose possible is given because of the potential adverse effects of these drugs on the fetus. These drugs easily cross the placenta to the fetus and may take a long time to clear from the baby's system even after birth. Many analgesics can cause respiratory depression (slowing of the breathing center in the brain) in mothers and babies if given in large amounts or in repeated doses.
Anesthesia--medications that cause loss of sensation include pudendal block, epidural anesthesia and analgesia, spinal anesthesia and analgesia, and general anesthesia.
Local block--anesthesia injected in the perineal area--the area between the vagina and rectum--numb the area for repair of a tear or episiotomy after delivery
Pudendal block--a type of local anesthesia that is injected into the vaginal area (affecting the pudendal nerve) causing complete numbness in the vaginal area without affecting the contractions of the uterus. The woman can remain active in pushing the baby through the birth canal. It is used for vaginal deliveries.
Epidural anesthesia (also called an epidural block)--this anesthesia involves infusing numbing medications through a thin catheter that has been inserted into the space that surrounds the spinal cord in the lower back, causing loss of sensation of the lower body. Infusions of medications may be increased or stopped as needed. This type of anesthesia is used during labor and for vaginal and cesarean deliveries. The most common complication of epidural anesthesia is low blood pressure in the mother. Because of this, most woman need to have an intravenous infusion of fluids before epidural anesthesia is given. Another risk of epidural anesthesia is a postpartum headache. It may develop if the epidural needle enters the spinal canal, rather than staying in the space around the canal. The anesthesiologist or nurse anesthetist will discuss the risks, benefits, and alternatives to the various methods of pain relief with the patient.
Epidural analgesia--this is sometimes called a "walking" epidural because the medication infused through the epidural is an analgesic, which relieves pain but does not numb the body and allows movement. Combinations of medications may be used in the epidural--part analgesic, part anesthetic. The most common complication of epidural analgesia is low blood pressure in the mother. This type of anesthesia is used during labor and for vaginal deliveries. Another risk of epidural analgesia is a postpartum headache. It may develop if the epidural needle enters the spinal canal, rather than staying in the space around the canal. Epidural analgesia may be used for pain relief in labor and for vaginal deliveries.
Spinal anesthesia--this type of anesthesia involves injecting a single dose of the anesthetic agent directly into the spinal fluid. Spinal anesthesia acts very quickly and causes complete loss of sensation and loss of movement of the lower body. This type of anesthesia is often used for cesarean deliveries.
Spinal analgesia--this involves injecting a analgesic medication into the spinal fluid to provide pain relief without numbing. Spinal analgesia may be used in combination with epidural anesthesia or analgesia. This may be used during labor for pain relief.
General anesthesia--this type of pain relief involves administering an anesthetic agent that causes the woman to go to sleep. This type of anesthesia may be used in emergency cesarean deliveries.

Connect with us:
Download our App: