Learn more about unifocalization
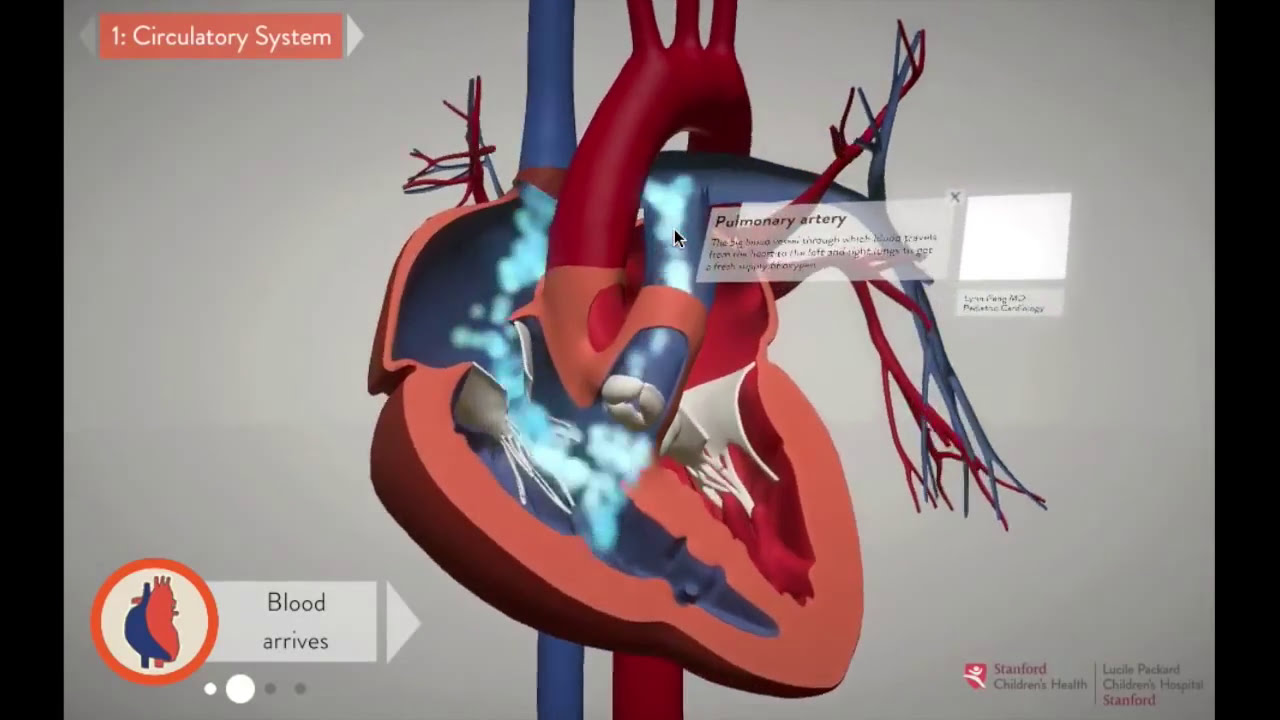
View the difference between a healthy heart and one with tetralogy of Fallot with pulmonary atresia and how our surgeons treat it with unifocalization.
Notice of West building lobby closure at Lucile Packard Children’s Hospital Stanford
A small number of newborns suffer from a complex and potentially fatal congenital defect known as tetralogy of Fallot with pulmonary atresia and major aortopulmonary collateral arteries. In infants with this defect, the blood vessels that should connect the heart to the lungs instead connect the lungs to the aorta, and the heart itself has a hole in the wall separating its lower chambers (ventricles). Our interactive 3-D animation helps you learn more about your child’s heart and unifocalization, a novel surgical technique, which we are number one in the world for performing.
In the past, heart surgeons could only repair this complex and life-threatening defect with several separate surgeries, each of which required the chest to be opened and the heart stopped. Unifocalization—developed and pioneered by Frank L. Hanley, MD, executive director of the Betty Irene Moore Children’s Heart Center—repairs the complete defect with only one surgery in the majority of patients.
Since pioneering unifocalization more than two decades ago, Dr. Hanley has fine-tuned it to improve patient outcomes for patients with a combination of tetralogy of Fallot (four defects in one) and other heart defects, as well as new conditions. For example, Dr. Hanley and the highly skilled team of cardiothoracic surgeons at Stanford Medicine Children’s Health are now using unifocalization techniques to better repair heart anomalies with major aortopulmonary collateral arteries (MAPCAs), including certain single ventricle conditions. Stanford Children’s is the number one program in the world for pulmonary artery reconstruction—unifocalization and other novel procedures.
View the difference between a healthy heart and one with tetralogy of Fallot with pulmonary atresia and how our surgeons treat it with unifocalization.
Operating on premature newborns with both congenital heart disease and very low (less than 1,500 grams, or 3 pounds, 4 ounces) or extremely low birth weight (less than 1,000 grams, or 2 pounds, 3 ounces) can be a difficult challenge because of their small size and immaturity. Conventional wisdom holds that it is better to wait for the child to develop further before undertaking heart repair. However, waiting can carry serious risks at times, because the heart defect leaves the child highly vulnerable to potentially fatal complications such as infection or lung disease.
Since fixing the heart defect as soon as possible can give your infant the best chance of living normally, the Betty Irene Moore Children’s Heart Center has developed surgical techniques for congenital heart defects even in extraordinarily small newborns, including successful repairs in the smallest, youngest infants known. As a result of this experience, the Moore Children’s Heart Center is among the world leaders in this demanding specialty.
The Moore Children’s Heart Center is one of the leading heart and heart-lung transplantation programs in the world and the only one that has had the highest volume of pediatric heart transplants in California for nine straight years. We specialize in providing transplants to children with complex health needs. To learn more about this treatment option, please visit Pediatric Advanced Cardiac Therapies (PACT) Program.
The highly complex Fontan heart surgery is performed on children born with a single heart ventricle. To correct this defect, a two-step heart surgery is often required within the first three years of life. The first surgery is the Glenn procedure, and the second surgery is the Fontan procedure.
About the Fontan procedure
The goal of the Fontan is to add a shunt (a small tube that improves blood flow in the heart) to allow blood to flow from the inferior vena cava (the main artery from the lower body) to the heart, and from there to the pulmonary artery and the lungs.
Our novel and superior approach to Fontan
There are four different types of Fontan procedures. At Stanford Medicine Children’s Health, we perform a unique off-pump extracardiac conduit Fontan without the use of a heart-lung machine (bypass), which results in better outcomes. Our survival rate for the Fontan procedure is 98%, despite treating children with very complicated needs who have often been deemed untreatable by other heart centers. Approximately one-third of our patients are referred to us from other heart centers around the country.
While the Fontan surgery does not return the heart to a perfectly normal state, it allows oxygen-rich blood to flow through the body, empowering children born with one heart ventricle instead of two to live an active, high-quality life.
Congenitally corrected transposition of the great arteries (CCTGA) is a rare and complex congenital heart defect that affects the structure of the heart. In babies born with CCTGA, the right and left ventricles are switched in position and in roles. As a result, the right ventricle must take on the more demanding role of pumping the blood to the body at high pressure. This puts a strain on the right ventricle, which in many cases leads to serious heart problems.
About CCTGA
Most children born with CCTGA eventually need heart surgery, and 90% of children with CCTGA have additional heart defects. For CCTGA, we carry out a complicated surgery that reroutes the blood within the heart and restores the roles of the right and left ventricles.
Our unique approach to CCTGA
We are one of a few programs nationwide that offer an anatomical “double-switch repair,” which our team of renowned heart specialists has been performing for the past two decades.
Our innovative, modified approach to the double switch not only reroutes the blood in the heart but also repairs other related heart conditions that your child may be experiencing at the same time. To increase success, we train (strengthen) the left ventricle before surgery.
Our unique approach to the double-switch repair, based on years of experience and research, has been shown to prevent or delay known major complications of the traditional double-switch repair. With our approach, your child can likely experience a better quality of life for longer; and in some cases, it can delay the need for another heart surgery.
Children with the congenital heart condition called anomalous aortic origin of a coronary artery (AAOCA) are born with one artery to supply oxygenated blood to the heart, rather than the usual two. Traditionally, AAOCA is treated with an unroofing procedure. At Stanford Children’s, we offer the more difficult reimplantation procedure to most of our AAOCA patients who need surgery for better close-to-normal anatomy and often greater success, as shown in our retrospective review of 230 patients under our care. Betty Irene Moore Children’s Heart Center is a destination for these patients, as our heart surgery team performs significantly more AAOCA repairs than many other pediatric centers nationwide.
At Stanford Children’s, we have become an international leader in surgical solutions for peripheral pulmonary artery stenosis (PPAS)—a rare, complex congenital heart defect frequently associated with Williams and Alagille syndromes (connective tissue disorders). Unlike pulmonary artery stenosis, which narrows the pulmonary valve, this condition narrows the smaller branches of pulmonary arteries, slowing blood flow to the lungs. Dr. Hanley has developed novel lung-heart surgical procedures for this condition, and we’re fortunate to have a team of highly skilled heart surgeons offering this new approach. Most centers favor catheter-based interventions. Instead, we use surgical reconstruction to improve long-term survival. Learn more in our retrospective review.
We are actively investigating ways of diagnosing heart rhythm problems while the fetus is still in the womb and performing corrective surgeries before birth. The Betty Irene Moore Children’s Heart Center is the world’s leading site for research in this area, led by Frank Hanley, MD.
The Moore Children’s Heart Center is actively involved in exploring new approaches to the surgical repair of pediatric heart disease and developing evidence-based guidelines for clinical care. We are often on the cutting edge of new devices, better surgical techniques, and ways to increase quality of life for children who undergo heart surgery.
Learn more about our groundbreaking research and innovation >
The hearts of children with complex heart defects are all unique, and heart surgery needs to be planned even more carefully. We have adapted cutting-edge engineering software to create custom digital tools for congenital heart disease—to improve outcomes. These innovative tools allow our cardiothoracic surgeons to create digital models of your child’s heart and blood vessels and perform virtual surgery before they enter the operating room, helping eliminate uncertainty.
These digital tools are especially useful for highly complex heart patients, including patients with single ventricle, heart failure, transplantation needs, pulmonary artery anomalies, and conditions requiring complex biventricular reconstruction.
We are likely the only center to have created tailored engineering software for CHD, and this heart surgery innovation has been shown to improve cardiac circulation and reduce the number of repeat surgeries.
If you would like to learn more or if you are ready to make an appointment, please call our team.


Connect with us:
Download our App: