Contact us
Contact us to learn more or if you are ready to schedule an appointment.
Notice of West building lobby closure at Lucile Packard Children’s Hospital Stanford
Stanford Medicine Children’s Health is a leader in surgical treatment for congenitally corrected transposition of the great arteries (CCTGA). We specialize in a modified version of the double-switch surgery, or anatomic repair, which is specifically used for individuals with CCTGA. CCTGA is also called L-TGA, atrioventricular and ventriculoarterial discordance, or double discordance. With CCTGA, the right and left ventricles are switched in position and in roles.
Based on our 20 years of experience and research, at the Betty Irene Moore Children’s Heart Center we’ve embraced the modified version of the traditional double-switch surgery (also called anatomic repair). We are one of a few programs nationwide that offer an anatomic solution to more closely re-create normal heart structure.
Anatomic repair allows the ventricles to perform the roles they were designed to do. This type of reconstruction restores the left ventricle of the heart as the pump to the body and the right ventricle as the pump to the lungs. In addition, our center performs a superior cavopulmonary (heart-lung) connection (also called a Glenn procedure) in most anatomic repairs. This removes some of the blood volume that the right ventricle needs to pump and lowers the pressure it needs to generate when pumping. In doing so, the right ventricle is less strained, which helps prevent serious heart complications over time.
Our modified anatomic repair with superior cavopulmonary anastomosis (Glenn) approach optimizes the function of the tricuspid valve and right ventricle. It also tends to diminish scar tissue in the atria (the chambers above the ventricles in the heart). With reduced scar tissue, there is less risk of problems with you/your child’s heartbeat and blood flow (complications called sinus node dysfunction, atrial arrhythmias, and baffle obstruction). It has also been shown to prevent or delay major complications associated with the traditional double-switch approach, the most common being weakening of the right ventricle or significant leaking of the tricuspid valve. When this happens, the heart can fail, or blood can back up within the heart, causing fatigue, shortness of breath, and an irregular heartbeat.
By decreasing the workload of the right ventricle and repairing other related heart conditions that you/your child may be experiencing (about 90% of babies born with CCTGA have additional heart structure abnormalities), you/your child can likely experience a greater quality of life for longer, and in some cases it can delay the need for another heart surgery.
There are two main types of anatomic repair, depending on your/your child’s anatomy—a modified double-switch surgery and a Rastelli-type modified double-switch surgery. When there are two normal-sized blood vessels leaving the heart, we generally offer the modified double-switch surgery, which involves performing three surgical procedures: hemi-Mustard, Glenn, and arterial switch. For individuals who have CCTGA and pulmonary stenosis or atresia, we perform a second type of modified double-switch surgery that consists of a hemi-Mustard, Glenn, and a Rastelli baffle (procedure) with an artificial connection between the right ventricle and lung, called an RV-PA conduit.
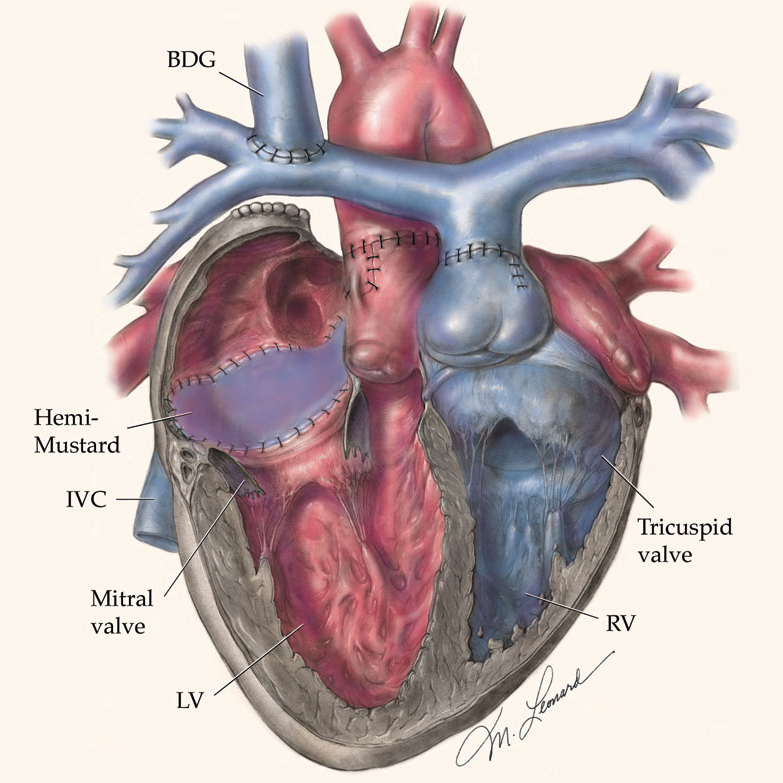
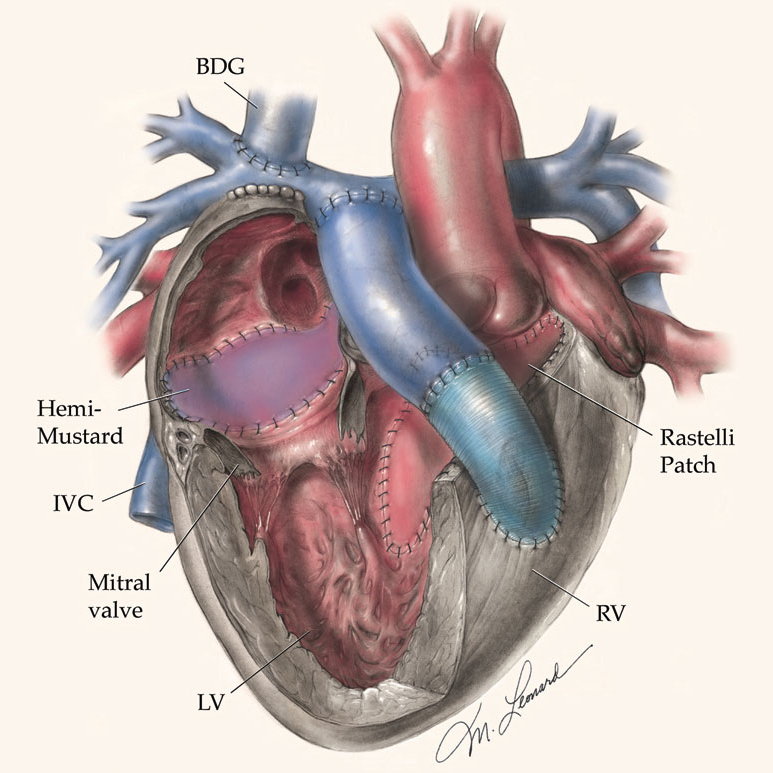
These diagrams show the two types of anatomic double-switch surgeries that we perform, depending on your/your child’s anatomy. On the left is the modified double-switch repair. On the right is the Rastelli-type modified double-switch repair, for patients with CCTGA and pulmonary stenosis or atresia.
Along with offering our modified double-switch surgery, we provide management of care for individuals with CCTGA. We have developed clear criteria to help guide care decisions for each patient, taking into account a patient’s unique condition and health needs. Together with your cardiologist, we individually tailor care over the span of your/your child’s lifetime to determine when and if surgery is the right next step and how best to enhance health and well-being. Our program has managed more than 100 patients with CCTGA in the last 20 years, a considerable number when only about 0.5% to 1% of babies born with heart defects in the United States each year are diagnosed with CCTGA.
Contact us to learn more or if you are ready to schedule an appointment.

Connect with us:
Download our App: